


Screening for breast cancer, Part 2
Why don't women do what's best for them? Maybe they do!
In my post “Screening for Breast Cancer”, I suggested that there are two different perspectives on health care decisions, the “medical care model” and the “public health model”.
I expanded on that idea in my next post, “Medical care, public health, and everything in between”, showing the “medical care model” and the “public health model” sitting at opposite ends of a spectrum, like this:
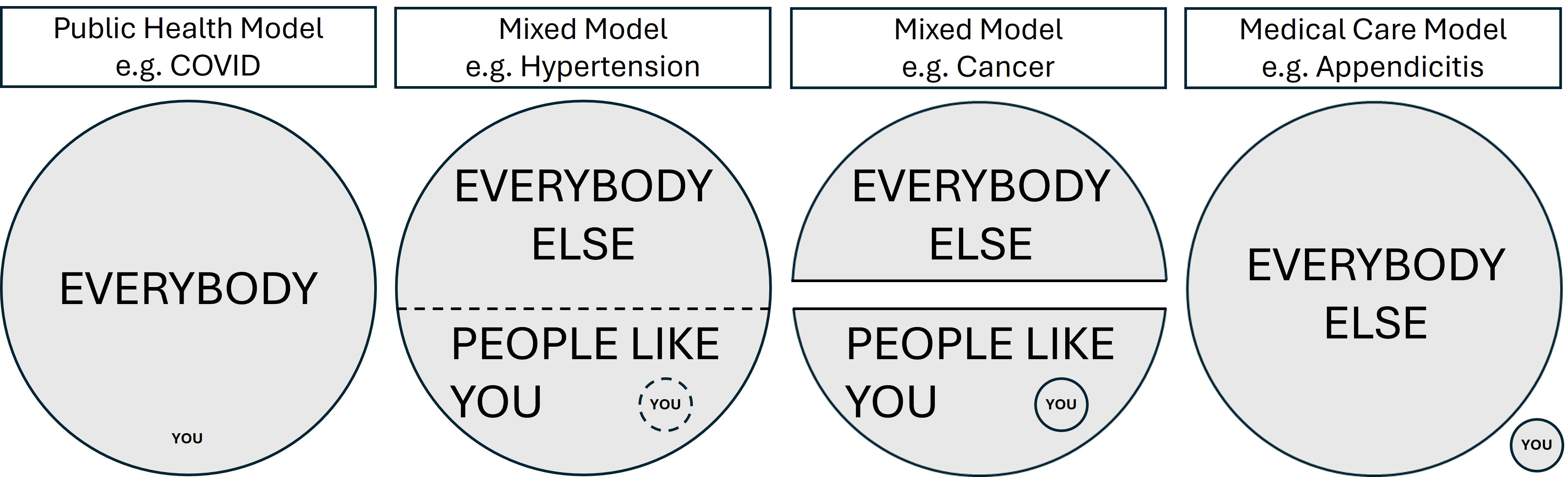
Toward the left, the public health model dominates, with population-based problems and their solutions defined in terms of statistical risks and mathematical models. Toward the right, decision-making reflects what’s best for the individual patient.
Importantly, the guiding ethical frameworks differ at the two extremes.
Public health ethics involve:
balancing the health of the community with individual rights,
developing and maintaining a relationship with the community,
addressing the fundamental causes of disease as well as the physical and social requirements for healthy communities, and
ensuring that public health measures are fairly imposed across the entire population.
Medical care ethics involve:
ensuring freedom of choice for individual patients and their health care providers,
weighing the potential risks and harms against the benefits, for everything they do to each patient,
acting only in ways that are beneficial for the patient, and
respecting individual rights.
In the middle ground, patients and their health care providers sometimes struggle to make informed shared decisions about their health care. In some ways, the differing ethical frameworks contribute to the problem.
In this post, I’ll explore this conundrum as it applies to breast cancer screening.
Breast screening, the benefits and the harms.
As with everything, there are benefits and harms in breast screening. Some are more common and/or more important than others.
On the harm side, we have:
the time spent booking the appointment, travelling to and from the facility, and actually having the mammogram.
the discomfort (or even pain) caused by the procedure itself.
the financial costs, including personal costs like missed time from work, travel costs and parking expenses, as well as the cost of the mammogram itself, which may be paid by the woman, her insurer or the government.
the anxiety associated with surrendering control to healthcare providers, having a procedure done, and waiting for the results.
further time, expenses, discomfort and anxiety for those women who have to return for additional views and/or biopsies.
radiation effects from repeated breast x-rays (these are reportedly very small).
over-diagnosis of the inoffensive or slow-growing cancers that were never destined to have significant consequences during the person’s life. It being impossible to separate these from the more serious cancers, the over-diagnosed patient is also over-treated, incurring:
needless investigations and treatments,
the inconvenience, costs and side effects of these investigations and treatments,
a cancer diagnosis (stigma, self-image, mental health effects), and
more frequent medical appointments to ensure the cancer does not reappear.
On the benefit side, we have:
the sense of reassurance that comes with a normal result, allowing for the fact that the reassurance is somewhat “false”. (Mammography does not detect all cancers; some are invisible on the mammogram and others develop in the interval between two mammograms).
earlier detection of breast cancer lesions, which are therefore smaller and in theory easier to treat (hence, less “aggressive” treatment at lower cost with fewer complications).
longer disease-free survival after diagnosis (which can be overstated due to “lead time bias”).
fewer breast cancer deaths (although women find other ways to die, so all-cause mortality doesn’t change as much).
That’s a lot to consider, so let’s put some numbers on it, using the following graphic from a recent Canadian draft decision tool. This pertains to the 50-59 age group, where the balance of benefits and risks is thought (by the experts) to clearly favor breast screening. The right side shows what happens to 1000 women who forego breast screening, as compared to the thousand on the left who are screened. Take a minute to ponder it. Remember, it’s supposed to be helpful.

Even though this tool is specifically designed to help people understand the statistics, it’s still pretty complicated, so let me break it down further:
Without any screening:
in a cohort of 1000 women aged 50-59, over a 10-year time span 980 women would NOT be diagnosed with breast cancer. That’s 98%!
Of the 20 who are diagnosed with breast cancer (presumably after they develop symptoms), only 3 will die of breast cancer during the 10 years. So, with or without breast cancer, 99.7% don’t die of breast cancer!1
Screening every two years detects an additional 7 breast cancers, at a cost of:
In the screened group:
only 1 or 2 would die of breast cancer during the 10 years, delaying “up to 2” deaths4.
973 people would screen negative and wouldn’t actually benefit from the screening.
The 366 called back for additional testing, including 46 biopsies, would arguably be harmed.
If you are a 50-year-old woman considering breast screening, all that screening over the 10-year span means that your individual chance of NOT dying of breast cancer increases from 99.7% to 99.8% (or maybe even 99.9%)5. I guess that’s OK, if you’re the one (or two) who don’t end up dying of breast cancer, but it’s not so great if you’re among the group who are over-diagnosed, or who suffer the anxiety of further testing and/or biopsies. It’s a crap shoot! You might be helped, you might be harmed, or you might simply be wasting your time. What’s more, the decision aid doesn’t even consider the “soft costs”, like anxiety, inconvenience, etc.
Because mammography is publicly funded in Canada, there’s also no mention of the hard costs for screening the entire group, which are considerable. It’s hard to get exact numbers, even for publicly funded programs, but a Statistics Canada publication, now a few years old, estimated the lifetime costs of biennial screening of women aged 50-74 to be $11,200 per woman (or $450 a year for their 25 years of screening6). A lot of assumptions went into producing that number. For the small number of women who saw their lives extended, that cost translated to over $100,000 per “quality-adjusted life year”.7 To some, spending other people’s money, that might seem be a good deal, but how many women would cough up $450 a year for 25 years to buy a lottery ticket that offered them a 0.1% increase in their chance to avoid death from breast cancer?
To screen or not to screen, that is the question! What the experts think.
For the experts, following a public health decision-making style, the decision about offering breast screening involves figuring out the probabilities of all those different harms and benefits, assigning a “value” to each one, then deciding if the total good outweighs the total bad for the entire population of eligible women.
One way to do this is to analyze the “cost effectiveness”, which assumes you can assign a dollar value to everything. Since it’s hard to name a price for things like inconvenience, discomfort, anxiety, and altered self-image, cost-effectiveness analyses often limit themselves to comparing actual health system costs to the perceived dollar value of lives “saved” or quality-adjusted life years gained.8
Beyond that limitation, there are often underlying unstated value-based assumptions. For example, is it more important to reduce the number of breast cancer deaths, or to avoid harming women with unnecessary diagnoses and treatments? How you answer that question determines what value you assign to deaths delayed versus women harmed. Those who simply want to reduce breast cancer deaths advocate for screening starting at a younger age, and more frequent screening, accepting the cost of increased false positives and over-diagnoses. Conversely, those who want to reduce false positives and over-diagnoses argue for more targeted and less frequent screening. Still others argue that the dollars would be better spent on something else!
In the end, public health ethics seek the balance between the needs of the population and those of the individuals, accepting that it’s OK to harm some in order to help others, as long as it serves the greater good.
Here in Nova Scotia (which is pretty typical for Canada), the public health way of thinking shows up in the recommendation that women aged 50-74 with no increased risk factors have mammography every 2 years.9 At the abstract community level, the experts have looked at the data, seeing what they interpreted as clear evidence that screening mammography in that age group is more helpful than harmful for the population as a whole. They could have recommended annual screening, but that drives up costs and false positives, so they compromised. They didn’t talk to individual patients, but their systematic review on values and preferences suggested that a majority of patients would agree, downplaying the significance of any “variability in patient values and preferences”.
This exemplifies the prevailing public health paradigm; they make the decision, so you don’t have to.10 They expect 70% of eligible women to heed their advice. Sure, some patients will benefit, and others will be harmed. That’s just the cost of doing business. It’s more than a bit “paternal”. Why wouldn’t women want it? It’s for their own good!11
To screen or not to screen, that is the question! What women think.
For you, as an individual, the screening decision is actually complicated!
For a start, most people seek help from their health care providers when they are sick. You initiate the contact and, in that way, provide consent for investigation and treatment.
Screening, on the other hand, is something that is recommended to you by the screening program and/or your provider. Screening is done when you are well, but it can harm you.
The screening transaction, therefore, is fundamentally different from your usual doctor visit. It’s one thing for your doctor to recommend chemotherapy when it’s aimed at curing the thing that’s making you unwell, your lung cancer. It’s you that benefits and you that’s harmed, and you get to decide whether the anticipated benefits outweigh the harms. It’s another thing entirely for your doctor (or the health care system) to recommend screening, which carries a measurable and predictable risk of harming you while offering only an uncertain, statistical chance of helping you.12
That uncertain chance that screening will help you depends on things like your age, genetic mutations, menstrual history, pregnancy history, breastfeeding history, breast density, personal history of breast cancer, family history of breast or ovarian cancer, previous radiation treatment, drug exposure (like hormones or diethylstilbestrol), physical inactivity, weight, and alcohol intake. Some people are at higher risk than others, ergo some people are more likely to benefit from screening than others.13
The chance of breast screening harming you, however, is pretty well random and evenly distributed across the entire population of women being screened. The risk is measurable and predictable at the population level, but we cannot predict which specific women will suffer which harms.
The expert advice that women outside the 50-74 age group and those at greater risk talk to a health care provider to see if screening is right for them shifts things more toward the medical care model, where it’s about personal choice and shared decision making.
For you, at any age, deciding whether or not to have a mammogram involves comparing your personal risk with all those different harms and benefits, getting a sense of how likely they each are, deciding which ones matter the most to you personally, and then deciding if the good outweighs the bad. Your healthcare provider can help you to understand the benefits and risks, but at the end of the day the choice you make reflects what’s important to you.
This paradigm is gaining popularity, and rightly so. After all, your decision NOT to have a mammogram doesn’t place anyone but you at risk. Some people are risk tolerant, others are risk averse, and that’s OK. If there’s any benefit to having the mammogram (and you define what’s a benefit), it’s your benefit. If there’s a risk of harm, it’s your harm, accepting that your concept of harm might differ from mine.
In the end, how many women decide to get screened?
According to the 2023 Annual Report for the Nova Scotia Breast Screening Program:
Only 37.1% of eligible women aged 50–74 have actually had a mammogram in the past 30 months, well below the national target of 70%. That participation rate has been declining since 2019.
The retention rate is also substandard, with only 20.4% returning after their first screening mammogram (target 75%), and only 57.0% returning after a subsequent screen (target 90%). Again, both figures have been declining.
All of which makes you wonder. If screening mammography is so obviously beneficial, especially in the 50-74 age group, then why are so many women going against the sage advice of the experts and choosing NOT to do it? Are we doing a good job supporting women to make their own decisions about breast screening? Are their decisions rational, are they being cavalier about their health, or are they simply uninformed?
Tellingly, breast screening programs track participation rates against targets. They simply assume that a certain percentage of women will reach the “right” decision (the one that involves getting a mammogram). To that end, the major goal of many programs is to increase participation rates.
However, if we truly support the right of women to make their own decision, then the metric should be something like “the percentage of women who feel that they were adequately informed about breast screening, were given the opportunity to make their own decision, and are satisfied with the choice they made (regardless of whether or not they chose a mammogram)”. Granted, that’s harder to measure and report.
Either way, we need to think about how individuals decide what to do.
How do people make decisions, in theory?
There are basically two ways of looking at how people make decisions.
The classical “rational” model assumes that people add up the benefits and costs involved in any given decision, then choose the option that has maximal “utility” for them.
In a way, this is how those public health people and expert guideline-development groups approach things. They look at the probabilities of all possible outcomes (good and bad) across the entire population, assign “values” to the various possible outcomes, and then total things up to see if the overall good outweighs the overall bad.
At an individual level, however, the math is different, and people aren’t so rational. There’s plenty of evidence to show that:
Individuals are risk averse; they are more afraid to lose what they have than they are excited about gaining something of roughly equal value.
People have trouble with probabilities; they overestimate the likelihood of good things which are actually unlikely (like winning the lottery) and underestimate the probability of bad things that are more likely to occur (like complications from a “simple” biopsy).
Emotions and fear play into these problems. Uncertainty about outcomes creates the fear of losing something, which leads to risk aversion. Excitement about winning leads people to buy extra lottery tickets when the jackpot is bigger, even though the odds of winning are worse.
The way in which the choice is framed affects the decision. For example, it makes a difference whether you are offered breast cancer screening as:
a routine preventative activity that you can opt out of, or
an optional risk reduction activity that you can choose to pursue.
In real life, why don’t women get screened?
There’s still quite a push from on high for more and better breast cancer screening. The idea that early detection is unquestionably good is pervasive.
Plenty of studies have looked at which women don’t get screened. Most focus on administrative data, like education levels, household incomes, racial identity, proximity to a screening centre, etc. They’re population-based and statistical; typical public health stuff, in other words! They don’t really explain why individual women make the choices they do, unless you believe that their race or family income pre-determines the decisions they make. Notwithstanding those limitations, these studies are used to inform different communication campaigns, or innovations like mobile breast screening clinics.
I did find one study looking at why women choose not to be screened. Using decision theory, the authors concluded that women who see themselves as healthy (and associate the health care system with illness) don’t choose mammograms, because they are avoiding the inconvenience of screening, the loss of control they feel when dealing with the health care system, and the risk of being found ill. Those who fear breast cancer (and see prevention as a way to maintain their health) choose mammograms. Either way, it seemed that the decision women make is the one that makes sense for them, based in their world view.
Interestingly, the authors of that study then went on to say that “Healthcare providers need to focus on moving women from the ‘current health’ to the ‘preventive health’ status quo. This can be done by clearly explaining cancer risk, the benefits of screening, and the procedures involved, being careful to consider fear of the unknown.” So, rather than accepting that women are making decisions that are right for them (and trying to understand and accept their value system), the conclusion was that any woman making the decision not to have a mammogram was “wrong”, presumably because they didn’t fully understand the risk of cancer and the benefits of screening. Re-education was put forth as the solution!14
Even if one accepts that education is the answer (and I don’t accept that premise), how does one clearly explain cancer risk, the benefits and harms of screening, and the procedures involved, taking into account fear of the unknown? How does a health care provider present the cold hard facts without introducing some form of bias, deliberately or unintentionally framing things up in the way that leads the patient to make the decision the health care provider wants? Is it even possible for a woman to make an informed choice, one way or the other, when there’s so much societal hype about the importance of breast screening?
One proposed tool is the patient decision aid, similar to that shown above. In theory, these provide balanced and unbiased information about the options and their outcomes (including benefits and harms) to support informed decision making. Decision tools are thought to be most helpful in situations with risky or uncertain outcomes, when there’s no single best option, the sorts of situations where patient decisions will differ depending on the patients’ preferences, values and life situation. Believe it or not, there’s an entire organization dedicated to setting standards for decision aids! External reviews of decision aids, however, often expose the underlying biases of the authors.
Interestingly, even though patient decision aids are supposed to be complete, balanced and unbiased, some experts remain concerned that some patients, having been presented with all the facts about breast cancer screening, still end up making bad choices, not in keeping with their own professed values. In other words, patients can’t be trusted to make their own decisions!
That being the case, some experts make the argument that it’s ethically acceptable to “nudge” patients by making deliberate changes to the way in which the options are presented or framed, the goal being to steer women toward screening. In their minds, it’s okay to present the choice in a balanced and unbiased way, as long as it’s clear that the decision to have breast cancer screening is the only rational choice. This gets us back to the public health model, favoring paternalism and coercion over shared decision-making!
In conclusion
As with any situation where people make their own decision, there is always a possibility that women will make decisions which do not appear to be in their own best interests, in this case the “risky” choice to forego the mammogram. While some hope to find their breast cancer early, through a screening mammogram, others choose to “live dangerously”, finding their breast cancer later, when it becomes a palpable lump or causes other symptoms.
In theory, those who wait for symptoms to develop should have more advanced breast cancers and higher rates of breast cancer death. In practice, lots of women don’t get screening mammograms, and yet there’s not much evidence to suggest that they suffer significantly worse outcomes. In the real world, breast cancer screening produces a fairly tiny improvement in the risk of death from breast cancer, with little or no change in “all-cause mortality”. Breast cancer treatment has improved steadily over the years, and the advantage conferred by early detection has become minimal, at best.
That being the case, when it comes to breast cancer screening, women already appear to be making reasonable decisions, under the circumstances. In the face of massive promotional hype over several decades, they’ve individually looked at the benefits and harms of breast screening, some more common and/or more serious than others, sought more information as needed, and decided where the balance lies for them. Some choose screening, but many choose not to bother.
Mammographic breast screening has been around for decades. It seemed like a good idea in the beginning. It’s been around long enough that few people even question whether it’s still a good use of resources. There’s pressure to increase the frequency, expand the eligible age groups, and change the modalities used, all of which would drive up costs (and harms).
At the same time, the benefits of breast cancer screening are decreasing, we’ve gained a better appreciation for the harms, and there are questions about the ethics of offering predictably harmful interventions to large swathes of the population when the benefits are limited to a few. The following graph, for example, shows that, since the introduction of breast cancer screening, early-stage breast cancers have increased massively, with very little decrease in the incidence of late-stage cancers. In other words, we are over-diagnosing (and, in all probability, over-treating) the slow-growing and indolent cancers (the ones that would never kill you) and yet NOT reducing the incidence of the more advanced cancers (which, after all, was the selling point for breast cancer screening). Other graphs overlay the breast cancer death rate, which started declining well before the introduction of breast cancer screening, with no obvious inflection point since breast screening came along.

I think it’s time to rethink the entire breast screening program, but that’s one man’s opinion. There are, however, powerful forces lined up on the other side of that argument.
Of course, a number of women in this age group can be expected to die over a 10-year time frame, mostly of things other than breast cancer. This US publication from 2008, for example, includes the following table:
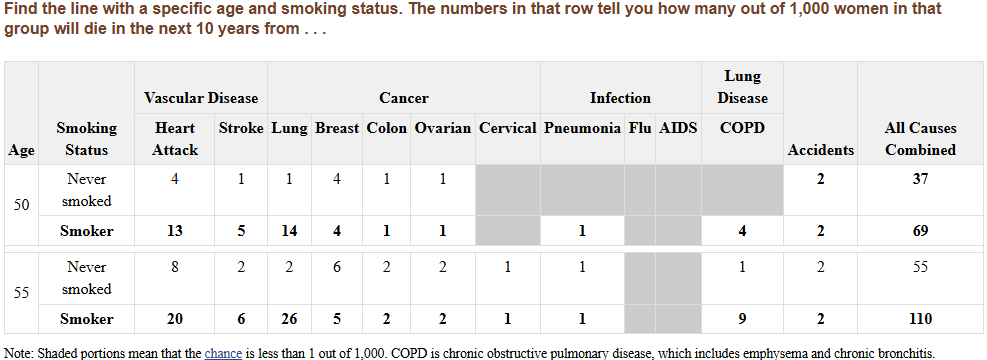
There being many ways to die, breast cancer might be the least of their worries!
(P.S. This table uses data from the early 2000’s and shows higher numbers of breast cancer deaths than the decision aid I’ve quoted in my post, reflecting the improvements in breast cancer treatment over the past two decades.)
For 1000 women over 10 years, a mammogram every two years means 5000 mammograms in total.
Many would argue that all 7 were over-diagnosed. I’m not sure how the developers of the decision aid decided it was only two. Estimates of over-diagnosis in the published literature range up to 50%, which, if true, would mean that every second breast cancer diagnosed through screening was over-diagnosed!
Because everyone dies in the end, I prefer to think of these things as “delaying death” rather than “saving lives”. We might detect and even cure your breast cancer, in which case you won’t die of breast cancer, but you’ll eventually die of something else.
The improvement in all-cause mortality is even less impressive.
The “lifetime costs” are incurred over the 25-year screening period, not the entire lifetime.
A 2013 cost-effectiveness analysis, published in the British Medical Journal, concluded that “The gain in person time survival over 35 years was 9.2 days per person and 2.7 quality adjusted days per person screened”. Obviously, in reality only a small number of people actually have their lives extended as a result of breast cancer screening, but what these authors are saying is that, if the added years of life were evenly distributed across all of the participating women, each woman would gain less than 10 days of life (over 35 years).
I’m not an expert in that sort of analysis (and to be honest I think that reducing everything to a dollar value is a clunky way to compare things as disparate as apples and monkeys) so I find these documents unreadable. For example, Cost-effectiveness of mammography from a publicly funded health care system perspective, concluded “The lifetime overall costs (undiscounted) to the health care system for annual screening per 1000 women ranged from $7.4 million (for women aged 50–69) to $10.7 million (40–74 yr). For biennial and triennial screening per 1000 women (aged 50–74), costs were less, at about $6.1 million and $5.3 million, respectively. The incremental cost–utility ratio varied from $36,981/ QALY for triennial screening in women aged 50–69 versus no screening to $38,142/QALY for biennial screening in those aged 50–69 and $83,845/QALY for annual screening in those aged 40–74. Interpretation: Our economic analysis showed that both benefits of mortality reduction and costs rose together linearly with the number of lifetime screens per women. The decision on how to screen is related mainly to willingness to pay and additional considerations such as the number of women recalled after a positive screening result.”
Other women outside those age groups or with other risk factors are encouraged to talk with their health care provider to decide when to start screening and how often to go.
As we saw during Covid, public health people struggle with letting individual citizens choose their own path. For the experts, it’s either “coercion” (lockdowns, mandatory masking, etc.) or “convincing” (where they give you a chance to make up your own mind but penalize you for making the wrong choice, as with the immunization requirements). They struggle with letting people have free choice.
The debate among experts gets heated when they start talking about women outside the 50-74 age group, or those with other risk factors. Some recommend more screening, others less. It all depends on the weights they assign to the various risks and benefits. Furthermore, politicians and advocacy groups start to weigh in, at which point it’s more about differing cultural values, and even less about the data.
Would you accept advice from your doctor to have your healthy breasts amputated (certain harm, not medically justified) because doing so would eliminate your future risk of breast cancer (possible benefit)? Is that the sort of thing your doctor should even be recommending? Where’s the balance between Beneficence (doing good) and Nonmaleficence (avoiding harm)?
When it comes to screening programs, at least one ethicist has built a pretty good argument that they are, in fact, unethical.
This Breast Cancer Risk Assessment Tool allows you to estimate your personal risk.
We’ll keep force-feeding you information until you feely choose the right option.
I don't get mammograms, quite simply, because I don't want my breasts squished in a vice! Ouch!! Lol. But I've read before that many of these screening tools are pointless and with the stats you've pointed out I'm even more certain of my decision. Great article, thanks.