

A lifetime of pain management, part 5
A lifetime of pain management, part 5
We're from Prescription Monitoring and we're here to help!
In my previous post, I talked about the various factors influencing the management of pain, one being “bureaucratization”. There’s just nothing like making things “overly concerned with procedure at the expense of efficiency or common sense”!
Consider prescription monitoring, for example.
In January 1992, the Nova Scotia Prescription Monitoring Program (NSPMP) commenced operations. We weren’t the first province to go down that path.1
The stated objective of the program was to curb the overuse, misuse and diversion of specific drugs, including opiates, barbiturates and amphetamines. The program later expanded to include anabolic steroids and benzodiazepines.
Most of those drugs aren’t used in pain management, so I’ll limit my further comments to the opiates.

There were very few electronic medical records in the early 90’s, and most prescriptions were handwritten.
The NSPMP introduced a triplicate prescription. Doctors didn’t have to use the form, but pharmacists could dispense the drugs only when the prescription was written on the approved form, which effectively made it mandatory. The prescribing physician retained one copy, the pharmacist another copy, and the final copy was forwarded to an agency (PMANS, the Prescription Monitoring Agency of Nova Scotia), where staff compiled the data manually.
In describing this history, the NSPMP website is somewhat confusing. (emphasis added).
Although PMANS was a voluntary association limited by its manual method of capturing prescription data on monitored drugs, it played a vital role in identifying the need to establish a legislative framework to support the operations of a prescription monitoring program. Consequently, the Prescription Monitoring Act was approved in October 2004 and subsequently proclaimed along with the Prescription Monitoring Regulations in June 2005. A Prescription Monitoring Board was appointed with the legislated mandate to establish and operate a prescription monitoring program for Nova Scotia. The objects of the Nova Scotia Prescription Monitoring Program (NSPMP) are to promote the appropriate use of monitored drugs; and the reduction of the abuse or misuse of monitored drugs.
So, it took them a decade, but eventually they realized that the bureaucratic structure they had created was in fact somewhat cumbersome! You also have to wonder what legal authority the NSPMP actually had for the first 12 years that it was in operation. The website suggests it was some combination of “policy guidelines” and “legislation”. Whatever it was, by 2004 they had clearly recognized that they weren’t on solid ground, and so the Prescription Monitoring Act was approved.2
After that, making a long story shorter:
a board was appointed, representing the College of Physicians and Surgeons of Nova Scotia, the Provincial Dental Board, the College of Pharmacists, the public, and the Department of Health and Wellness (DHW).
The DHW funded the program.
A private company, Medavie Blue Cross, administered the NSPMP.
by the end of 2007, all community pharmacies were submitting data through an on-line system, so the triplicate prescription pad became a duplicate prescription pad (one copy for the doctor, one for the pharmacy, with the pharmacists now doing the manual data entry).
in 2012, they launched a 24/7 online “app” (eAccess), allowing prescribers and pharmacists to access the most recent 18 months of a patient’s prescription history prior to prescribing and dispensing monitored drugs. (Previously, you had to phone and request the information from a staff member, but this innovation downloaded that work to the doctors and pharmacists.)
in 2016, NSPMP fully integrated with the provincial Drug Information System (DIS) to transmit monitored drug claim information multiple times per day.
in 2018, benzodiazepines were added into the program.
over time, so they say, they’ve adapted their safe prescribing protocols, reflecting the needs of people with chronic pain and addictions.
In all of this, there are several points worth considering.
The purpose was to fix a problem!
First, the NSPMP was set up to curb the perceived overuse, misuse and diversion of various drugs, opiates among them.
“Overuse” literally means using something “too much”. I suppose the founders had evidence that opiates were prescribed more than they should be. You can imagine that the program would, therefore, '“red flag” prescriptions that seemed excessive.
“Misuse” means that something is used in the wrong way or for the wrong purpose. Perhaps the founders had evidence that opiates were being prescribed wrongly (i.e. wrong drug, wrong dose, wrong frequency, wrong duration, wrong route, etc.), or for the wrong reasons. The prescription form, in its original format, didn’t ask about the diagnosis3, so it would be hard to know if the drugs were being prescribed for the right conditions. As for the dose, frequency, duration and route, that’s the sort of stuff that every pharmacist should have been reviewing on every prescription, even before the NSPMP came along.
“Diversion” means that drugs intended for one person were being used by someone else. However, there’s nothing about a triplicate prescription that stops the recipient of the drugs from “gifting” them to an acquaintance.
A 2014 review of Canadian Prescription Monitoring Programs4 claimed that “…the primary goals of these programs are to promote effective pain management while reducing prescription substance abuse….” However, despite that claim, the NSPMP didn’t start out with a mandate to promote effective pain management, nor was it ever designed to support that task. It was a prescription monitoring program, not a pain management program.
But was there a problem?
The NSPMP didn’t look at all pain drugs, it looked only at opiates. Clearly, they believed that overuse, misuse and diversion of opiates was a problem. You might ask what actual evidence they had to support that belief, but that’s hard to come by.5 All I’ve been able to find is the following, showing that, in 1994, 13.1% of the population nationally (13.3% of the population in the Atlantic Provinces) reported using prescription “pain pills” in the preceding year, leaving unstated how many of those pain pills were prescribed to the person who used them. Granted, that’s 1-person-in-8, which seems high, considering that children and teens wouldn’t often get prescription pain meds.

The solution to the problem.
Beyond “monitoring”, how is the NSPMP supposed to affect overuse, misuse and diversion of opiates, and what are the potential downsides? An economist explained it as follows (PDMP = Prescription Drug Monitoring Program, emphasis added):
PDMPs act as a negative supply shock for legally-obtained prescription opioids by making it more difficult for abusers to obtain prescriptions.
Former doctor-shoppers may turn to the black market for diverted opioid prescriptions because illegally diverted opioids are a substitute for legally prescribed opioids. The PDMP should therefore cause an increase in demand for diverted illegally-obtained opioids. However, the supply of diverted opioids available for purchase on the black market should also be affected by the PDMP because much of the supply of diverted opioids is obtained by doctor shopping, which the PDMP targets. Since the PDMP causes a decrease in supply as well as an increase in demand in the black market for illegally-diverted opioids, quantity effects are ambiguous and it is not clear whether police will encounter fewer or more illegal opioid crime incidents.
What he’s telling us is that these programs simply limit the supply of prescribed opiates, which could be used for pain relief, recreational purposes, or to feed addictions. They do nothing to limit demand. Assuming that demand remains the same, people will turn to the unregulated (non-prescribed) drug market, where they can find illegally diverted pharmaceuticals and illegally manufactured opiates (like heroin). In terms of overall societal use of opiates, anything could happen!
The effect on the doctor-patient relationship.
For family physicians (and others), the imposition of the NSPMP was a clear shift away from individual doctors prescribing to individual patients, according to their needs. It fundamentally changed the doctor-patient relationship and added work to each encounter.6
The benefits were for society, not the individual patient. With or without legal backup, the powers that be had decided that the societal harms of opiates justified collecting personal information for each and every opiate prescription.
No longer were doctors accountable to themselves, their ethics, their patients, their pharmacist colleagues, and their licensing body. Now, “Big Brother” was looking at each and every prescription.
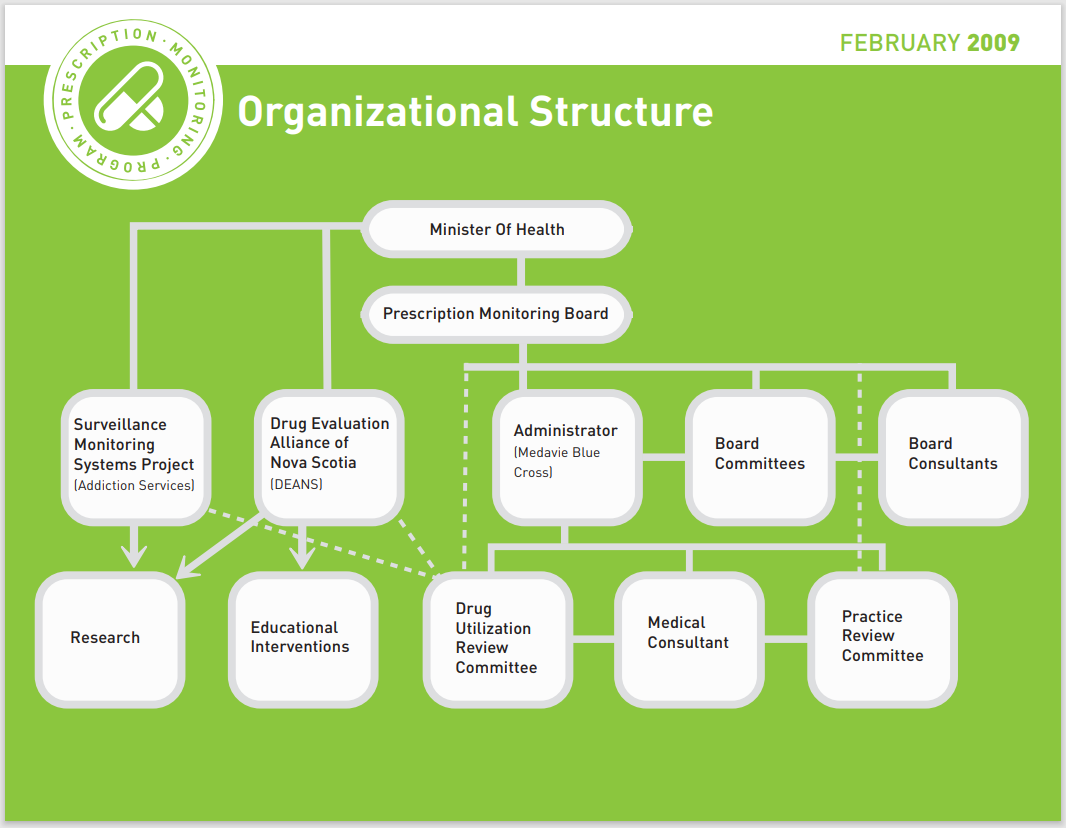
And who is Big Brother? In Nova Scotia, based on the current version of the NSPMP organizational chart, it’s the Minister of Health! The Prescription Monitoring Board reports to the Minister of Health. The program is administered by Medavie Blue Cross, who are hired by the Department of Health, and they work for the Minister.
Elsewhere in Canada, Big Brother is the provincial College of Physicians and Surgeons, which makes more sense. After all, the Colleges license physicians, investigate and resolve physician-related complaints, monitor and maintain standards of practice, and support high standards of medical practice and ethical conduct.
What does the NSPMP do with the data?
They monitor it and share it, of course!
Information about individual patients is shared with prescribers, pharmacists, police (through a defined process), and the patients themselves (upon request).
Information about the profiles of prescribers, pharmacies and patients can be shared with the various licensing authorities. For example, the physician profile is used when the Practice Review Committee of the College has a concern about an individual prescriber.
Doctors can request a prescriber peer comparison report, comparing their individual prescribing information with that of their peers in the same community, scope of practice (i.e. pain clinics) or medical specialty.
The NSPMP also share aggregate anonymous data on request with the media, prescribers, researchers or third-party insurers.
So, at least in theory, there’s a whole lotta sharing going on! That’s scary!
Maybe some examples will help:
eAccess provides 24/7 Internet access, so doctors can see what other prescriptions the patient recently had filled, prior to writing another prescription. This presumably prevents double-doctoring as well as inadvertent overdoses and/or drug interactions.
“Double-doctoring” messages are sent in real time to the pharmacy when a patient has had another prescription written by another prescriber and filled within the past 30 days at another pharmacy.
“Multiple prescriber reviews” are system-generated reports run every 28 days. These identify individuals who have seen three or more prescribers. Letters are then sent to all prescribers who have seen the patient, for information purposes.7
The “drug utilization review analysis” is a system-generated report run every 56 days. It identifies cases where the opiate doses and/or quantities exceed a proprietary threshold. Letters are sent to prescribers in potential cases of concern, and a response is required.8 The explicit threat is that the doctor could be subject to discipline if they fail to reply and/or their explanation is unsatisfactory.
Where trends in the aggregate data revealed patient safety issues, the data is shared in “educational settings”.9
Did it work?
You might be thinking that this all sounds good.
The powers that be recognized a problem with prescribed opiates.
They put in place a Prescription Monitoring Program. Paperwork!
They enhanced that program over time. They even made it legal!
They have a budget, a Board, subcommittees, procedures and processes, data and staff, including data analysts. A genuine bureaucracy!
They produce annual reports and strategic reports. More bureaucracy!
How well did it work? What did we taxpayers get for our money?10 Was it worth the intrusion on the physician-patient relationship? Most importantly, have we fixed the overuse, misuse and diversion of opiates?
Sadly, the NSPMP Annual Reports don’t really answer those questions.
They don’t tell us how many prescriptions were written or what quantity of opiates were dispensed. They don’t say whether these have changed over time.

To my eye, on a population of a million people, with 1-in-8 using opiates, that number of reports, reviews and referrals seems pretty low, and there are no obvious trends. The sad truth is that there’s really not a whole lotta sharing going on, and certainly not as much as there should be, if there’s a problem.
Those eAccess Patient Profiles are supposed to be used at the point of care each time a prescription is written or dispensed, but they are only generated a few thousand times a year. This is alarming, because as of 2017, over 35,000 people received prescribed opiates in each quarter of the year. I guess this is why the NSPMP 2023-26 Strategic Plan says, in an understated fashion, “Although the NSPMP has been active for some time, awareness of the program is often overlooked or misunderstood. NSPMP will explore various information channels to increase awareness and understanding of Nova Scotia’s prescription monitoring program’s role in supporting patient care, harm reduction and public safety.”
Supposedly, a major advantage of the NSPMP is the ability to track trends in prescribing, including the identification of variations in opioid prescribing by region, population density, sex and age. It’s not clear from the NSPMP Annual Report, however, whether this was done, or what use they made of that data. Presumably, it would inform targeted education, but they haven’t described any, nor have they shown the benefit of any education.
What about diversion? According to that 2014 review article, the NSPMP had “virtually eliminated” double doctoring by 2011, when there were only two charges for double doctoring in Nova Scotia. The NSPMP annual report for the last few years shows zero referrals to law enforcement. However, we don’t know how much double doctoring there was before. Anecdotally, I have heard that allegations of double doctoring are actually quite difficult to prove, which might explain the paucity of referrals and charges. And then there’s the following, which comes from a “confidential” Nova Scotia Drug Report that I stumbled upon on the Internet, showing that the majority of opiate drugs seized by police were “pharmaceutical”, suggesting that diversion is still a problem.

Having all that data could support the evaluation of the impact of any “interventions” initiated by the prescription monitoring program, showing what measurable effects they’ve had on opiate use. Alas, they’ve neglected to share that with us.
Looking elsewhere, I did find a research paper looking at NS opioid prescriptions for the 2011-17 timeframe.

The good news is that less than 5% of the population were dispensed a prescribed opioid, and that number is dropping. The bad news is that the Canadian Alcohol and Drug Use Survey of 2019 (which is the successor to the Alcohol and Other Drugs Survey of 1994 that I quoted above), contains the following graph, showing that Opioid Pain Relievers were still used by 14% of the population, slightly up from 1994! If 5% of the population are sharing their prescriptions with another 9%, that’s a lot of diversion!

Maybe it could have been worse!
The standard logic in opiate circles is that programs like safer supply don’t necessarily make things better. They work by preventing things from getting worse.
Maybe NSPMP can claim to be a success, by virtue of the fact that things didn’t get worse?
That 2014 review article contains the following quotes:
“The mere presence of a prescription monitoring or review program cannot stop diversion, misuse or addiction to prescription drugs because these complex problems are multifactorial. The effectiveness of a program can be measured in terms of prescribers’ and dispensers’ behavioural changes, promotion of safe and healthy prescribing habits and collaboration among all involved parties.”
“Although it seems intuitive to believe that nonmedical use of opioids may be higher in provinces without prescription review/ monitoring programs, the lowest Canadian levels are found in Quebec, which does not operate a program. In addition, Fischer et al showed no temporal changes in overall prescription opioid use by provinces that had a prescription monitoring program in existence.”
So, there you have it! The original objective to stop diversion, misuse or addiction was unrealistic! PMP’s don’t alter opiate use! We should be happy that we’ve altered behaviour, even without proof!
OK, perhaps they work elsewhere!
Nope! BC has the worst opiate problem in Canada, and they were the first to have a PMP. Quebec was the last to set up a PMP, while their opiate problem is nowhere near as bad as the rest of the country.
A 2019 systematic review of PMPs, funded by the Canadian Institute of Health Research, looking at the entire world literature, concluded that any reduction in the actual number of prescriptions is simply due to the added paperwork. Beyond that, there’s no proof that PMP’s “work”.11
“Studies showed that multiple copy prescription program (MCPPs) were associated with a decrease in the prescription of Schedule II medications; this decrease was due to inconvenience rather than an increased awareness of appropriate prescribing.”
“Evidence of effectiveness of interventions targeting the prescription of opioids is scarce in the literature. Although PMPs have been associated with a reduction in the overall prescription rates of Schedule II opioids, their impact on the appropriateness of use taking into consideration benefits, misuse, legal and illegal use remains elusive. Our review suggests that existing interventions have not addressed all determinants of inappropriate opioid prescribing and usage.”
In conclusion…
The Nova Scotia Prescription Monitoring Program (and every other PMP) is a classic example of bureaucratization. Costs money. Makes work. Accomplishes little or nothing! Well entrenched. Good luck getting rid of it!
Alberta and Saskatchewan were ahead of Nova Scotia. Most of the other provinces came later, except for Quebec, which is only now getting around to it.
In the United States, all 50 states implemented online electronic drug histories between 2004 and 2016, although some had been tracking the data on paper for decades.
The current version of the Act makes no mention of any pre-2004 legislation.
They did remedy this omission at a later date, requiring the diagnosis to be written on each prescription.
I highlight this article as it summarized four PMPs across Canada, Nova Scotia among them, with two of the authors being associated with the NSPMP (i.e. “insiders”.
I’ve searched high and low for data on opiate prescribing in Canada in the early 90’s, and I can’t find any. Most of the published data starts in the early 2000’s and makes reference to the fact that there was no reliable prior data. There’s nothing more bureaucratic than setting up a program to FIX a problem when you have no reliable data to say that there actually IS a problem!
We were supposed to store the prescription pads in a secure location, so we would have to fetch a prescription form and then legibly fill in ALL the boxes on the form, including a lot more information than you would have on any other prescription. For people like me, writing legibly is time-consuming. I happened to be using electronic medical records at the time, so all my other prescriptions were machine-printed.
Sometimes, this is unsurprising, as when a patient went to emerg with an injury, gets an opiate prescription, sees a specialist and gets a refill, and then sees their family doctor at a later date for another refill. At other times, this might be unexpected, triggering a conversation with the patient about their sourcing and use of opiates.
The thresholds the program uses are for internal purposes only and are not shared with prescribers, to prevent the behaviour of prescribing to a dose immediately below the threshold. They are developed by a committee of experts and are reviewed and revised regularly.
This is a bit like putting a speed camera on a road with no posted speed limit. You check the speed of every car and then ask selected drivers to explain why they were driving “too fast”.
The educational example they describe relates to meperidine (Demerol), which should not be used long term, due to the accumulation of a harmful breakdown product.
The current NSPMP budget is about $1.5 million per year. Assuming that’s been fairly constant over the years (while growing with inflation), that means they’ve spent nearly $50 million since the program was set up.
A conclusion which was duplicated in other recent systematic reviews.
I live in a place with zero prescription oversight, of any type, and where double doctoring is accepted as the norm. People here will have GPs, by condition, or use specialists as GPs. There is no visibility into what has been prescribed by anyone for anything. We are looking to provide visibility. But it is the other end of the spectrum. I don’t think it is better. Where is the right answer?
Very interesting again Rick. I didn't know this history.
In the last few years, a number of experts have lauded the decrease in opioid prescribing as a success in education and safety. But IMO this decrease has been offset by an increase in other drugs like Gabapentin/Lyrica/etc. The urge to fill people with pills until they stop complaining to us doctors is still strong in modern medicine.